Multidisciplinary Team Working to Address New Trends in Opiate Use Disorder
Medetomidine-associated withdrawal presents extreme symptoms requiring innovative treatment pathways to standardize care

Hospitals across our region are seeing rapid changes in opiate use disorder as the drug supply continues to shift. Over the past several years, xylazine, a veterinary sedative, emerged as an additive in the fentanyl supply. As an alpha-2 agonist, xylazine causes severe ischemic wounds and requires more surgical and wound care resources.
About a year ago, clinicians began noticing fewer wounds and an increase in extremely severe withdrawal, including profound vomiting, diarrhea, and blood pressures higher than seen before in this population. This shift coincided with the emergence of medetomidine, another veterinary sedative and alpha-2 agonist estimated to be 100 times to 200 times more potent than xylazine. The substance has been identified in the regional drug supply spanning Delaware, Philadelphia, Pennsylvania, and the surrounding areas of Maryland and New Jersey.
Severe Withdrawal and Clinical Impact
Medetomidine-associated withdrawal includes intractable vomiting, severe hypertension, tachycardia, agitation, and tremors, which can lead to strokes, posterior reversible encephalopathy syndrome (PRES) and seizures. Traditional opioid treatments do not improve these symptoms, requiring the use of alpha-2 agonists such as clonidine.
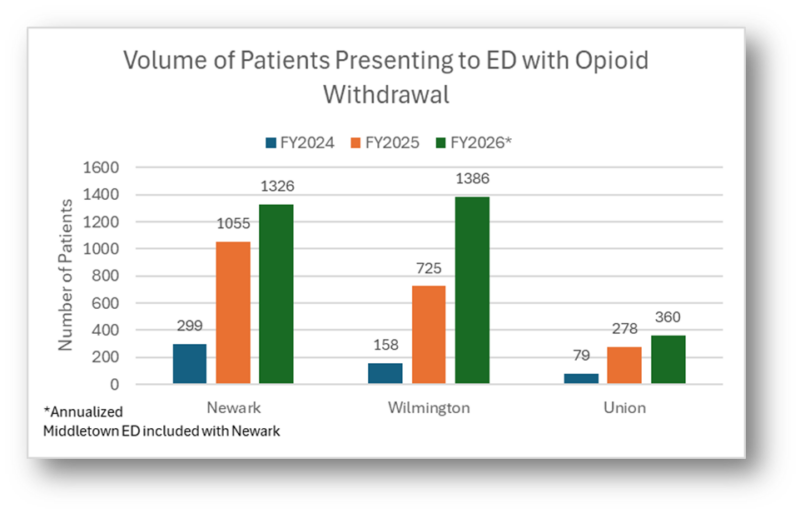
Often the intractable vomiting is so severe, that only IV medications are effective, resulting in a significantly larger number of patients requiring admission. These patients often require dexmedetomidine infusions, traditionally reserved for sedation in the ICU to help get symptoms under control before they can be stable on oral therapy. This new disease process has become the predominant utilization of our step-down beds and even ICU beds, at times occupying up to 50% of the units. The data below shows the rise in volumes we have been experiencing over the past two years across all campuses.
Standardizing Care
Recognizing the strain on inpatient resources and caregivers, a multidisciplinary group – including emergency department leadership, addiction medicine, hospitalists, pharmacy and clinical effectiveness– are working to understand this new disease process and on creating new treatment pathways to standardize care.
Key updates include:
- A new ED order set supporting guidance for initiation of partial opioid agonist treatment, reducing reliance on opioids, and aggressively treating profound vomiting with several anti-emetics to help start treatment early and get symptoms controlled more quickly.
- Expanded use of clonidine and benzodiazepines to minimize the need for dexmedetomidine infusions and help with the extreme agitation.
- A new medetomidine-specific order set more appropriate for medetomidine withdrawal, with criteria for escalating doses quicker to stabilize patients, weaning quicker, hypertension management support and a two- to three- week clonidine taper to guide transition into oral therapy.
Supporting Caregivers and Safety
With caregiver stress, safety risks and inpatient overdose concerns on the rise, all three campuses have implemented strengthened safety protocols to improve outcomes. These include:
- Removal and secure storage of belongings.
- Searches when paraphernalia is suspected.
- Visitor restrictions when needed.
- Support from public safety and a new patient expectations handout.
When the workload was reviewed, it was discovered that nurses were spending more time at bedsides for these patients than some ICU patients required. Campus nurse leaders have adjusted step-down unit nursing rations, with further ED nurse staffing needs under review for improvement. Maureen Leffler, D.O., MPH, chief well-being officer, continues to evaluate the impact on caregivers and expand support resources.
Community Partnerships and Transitions of Care
To improve long-term outcomes, ChristianaCare is strengthening relationships with expert community partners specializing in group therapy and wraparound services for these patients. Together, communication and the leverage of resources can occur. The community health and population health teams are improving access to clinical care through the Hope Center, mobile van, and access to primary care allowing these programs to take patients despite medical complexity.
ChristianaCare is also working with residential programs to create more bed-to-bed transfers, supporting safer transitions of care and better continuity of care to work on the psychosocial challenges many of these patients face.
Looking Ahead
Just as COVID-19 required rapid adaptation, this evolving phase of opiate use disorder demands new clinical approaches to adapt. Though currently regional, medetomidine is expected to spread nationally. Our caregivers, leaders and clinical partners continue to innovate and pioneer treatment guidelines to refine care processes with the expected ongoing drug supply changes.